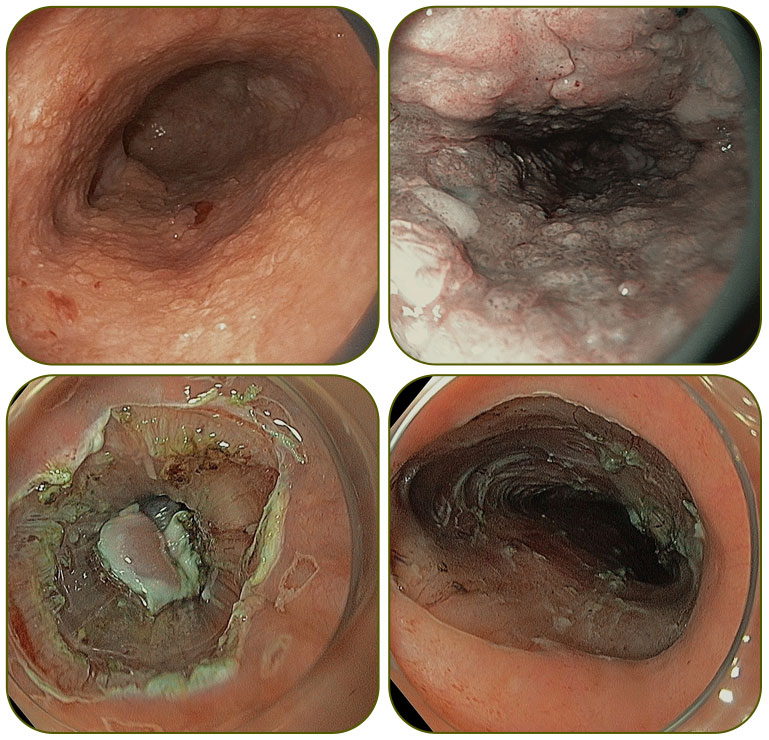
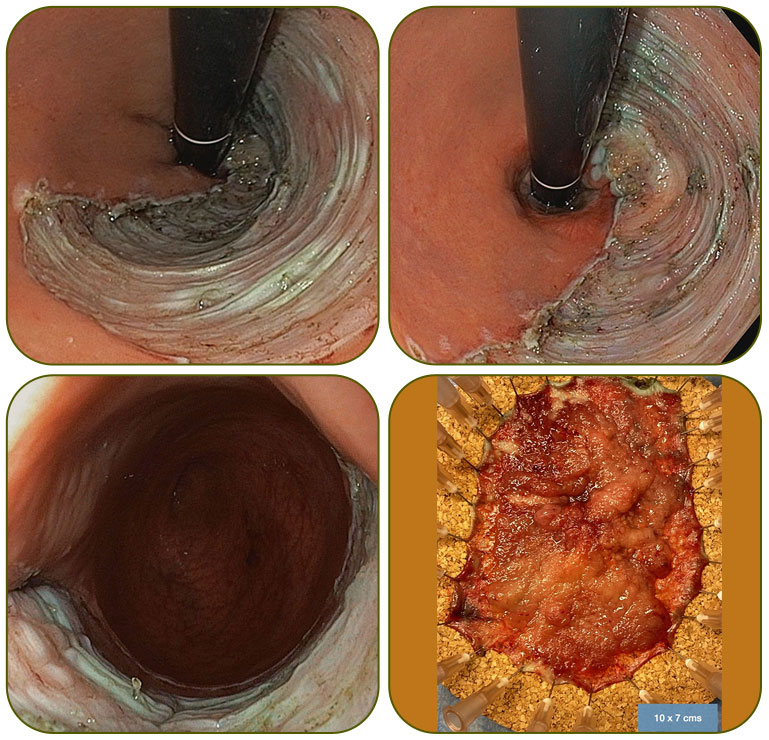
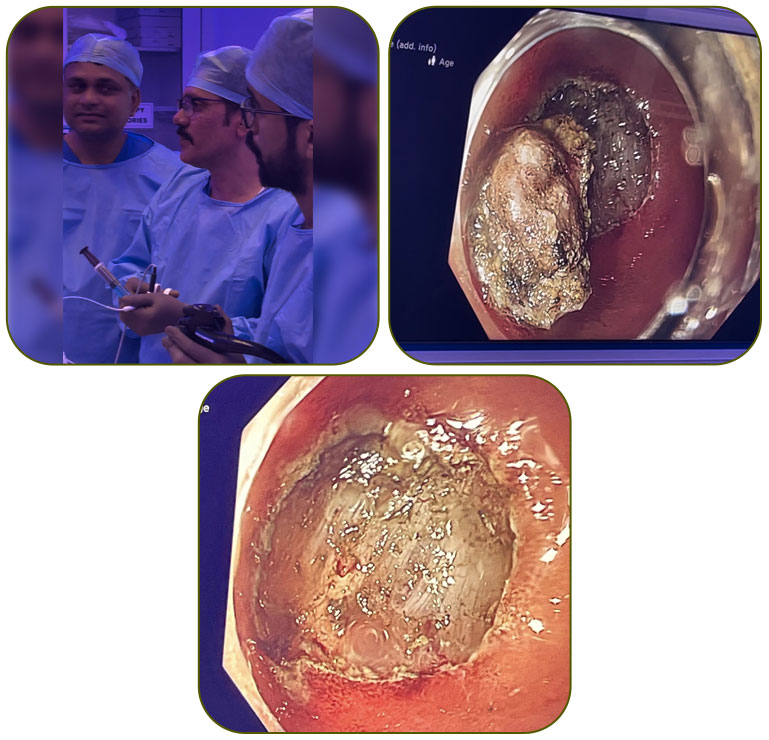
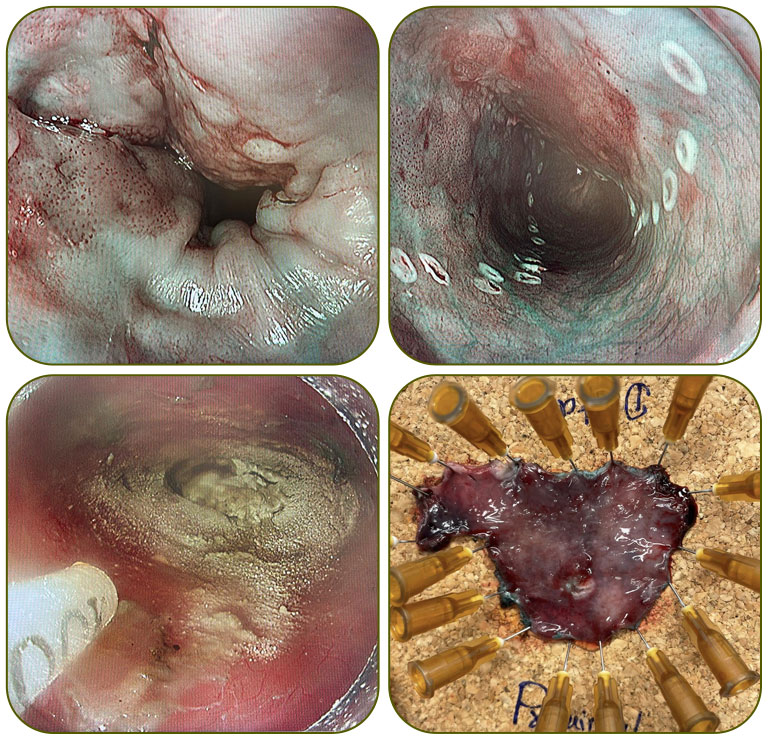
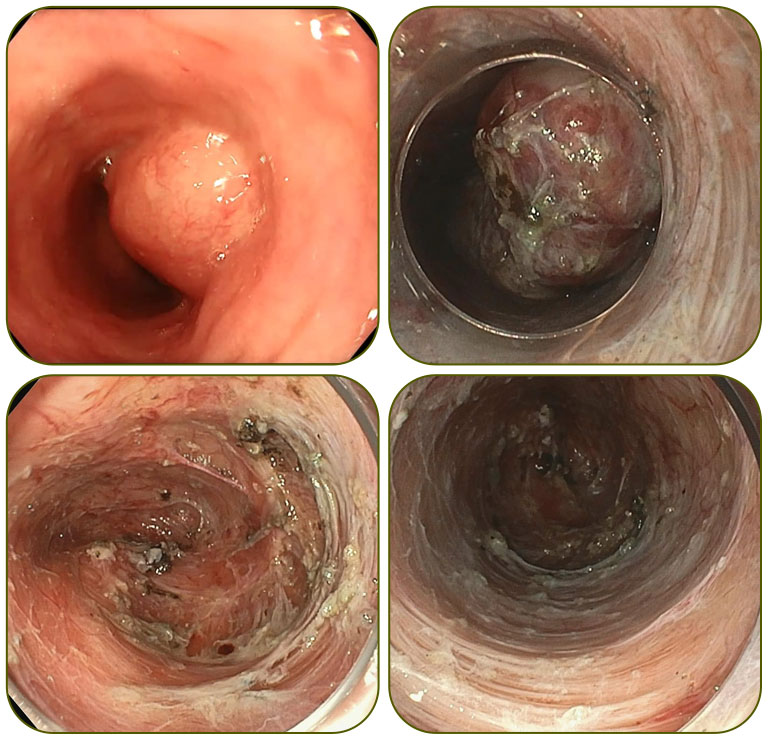
A long-segment (~10 cm) esophageal lesion with high-grade dysplasia managed with circumferential ESD - Endoscopic Submucosal Dissection.
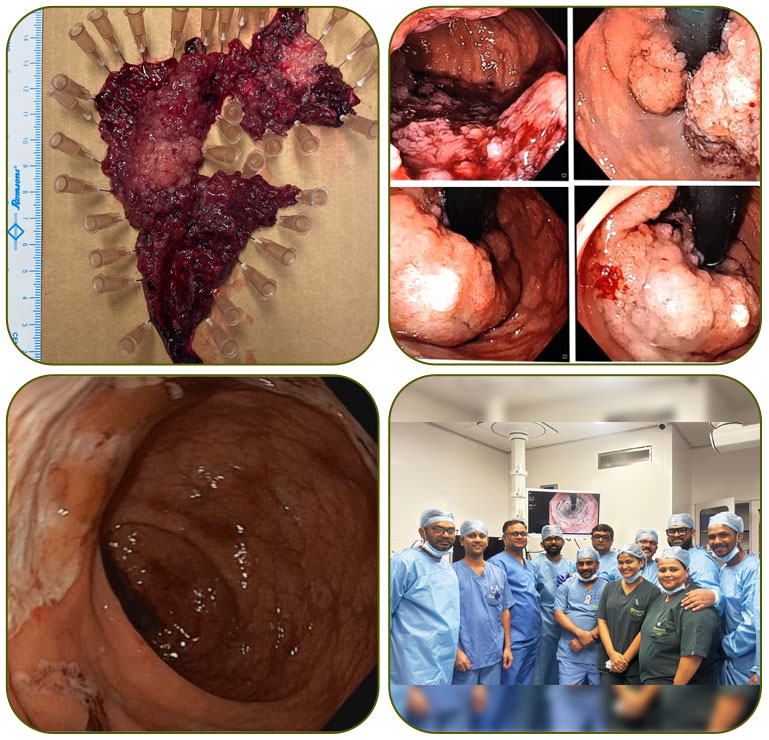
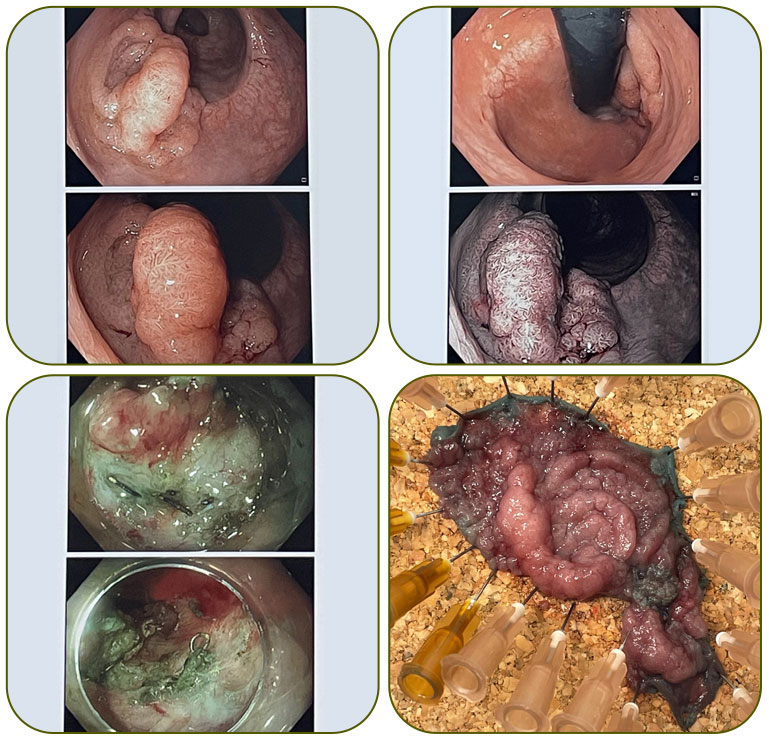
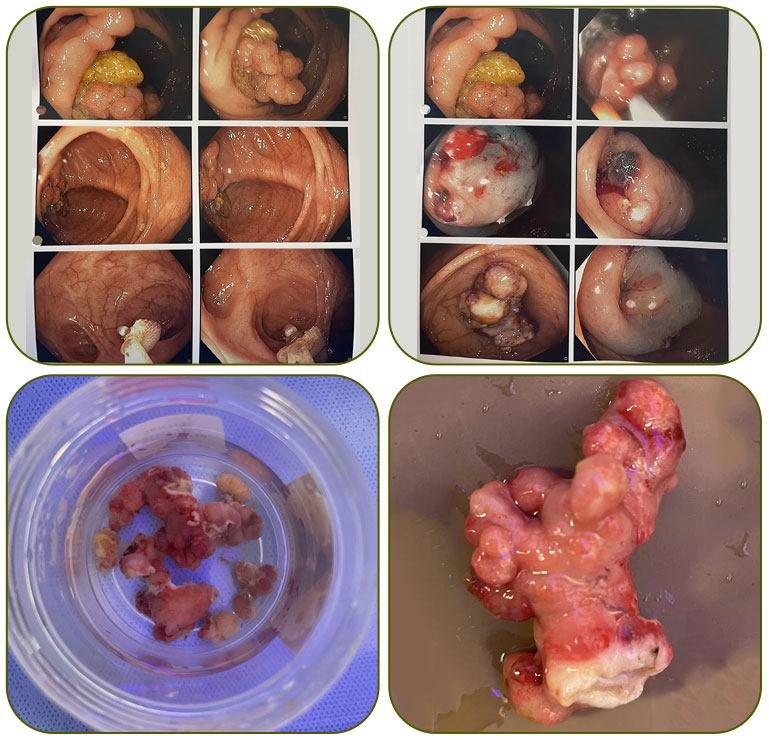
Large Rectal tumor LST-G (mixed nodular), starting from the anal verge and extending up to 8 cm. Successfully treated with endoscopic surgery.

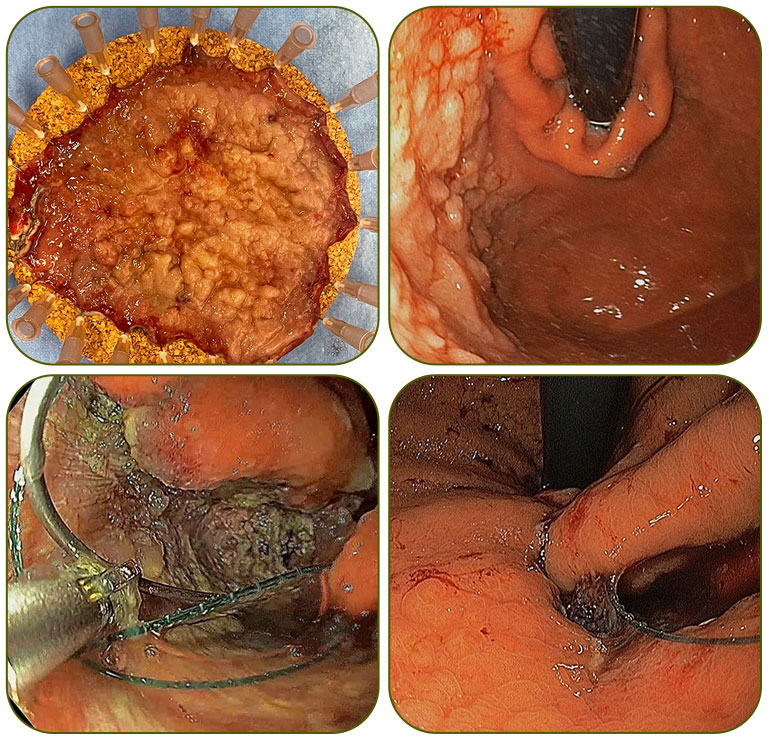
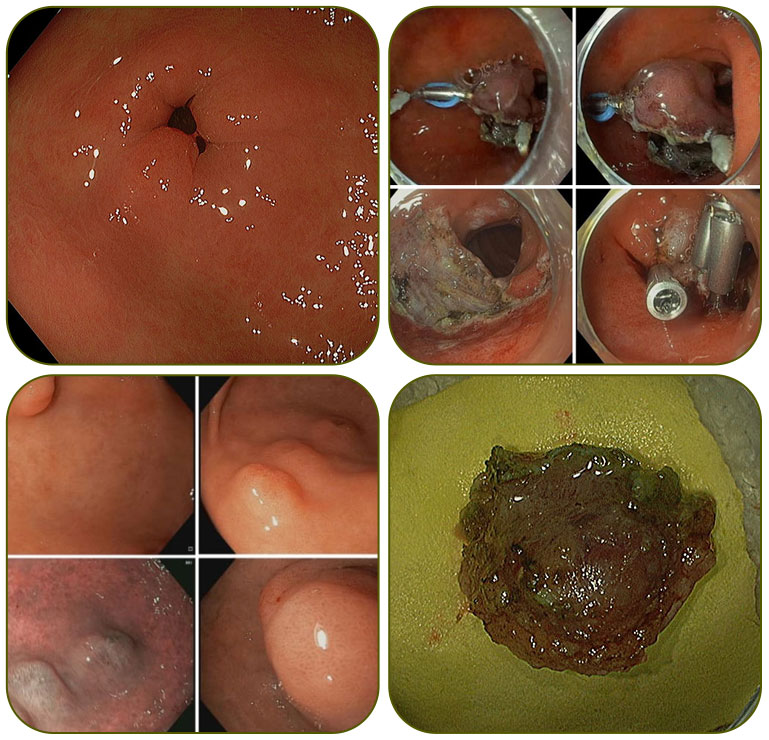
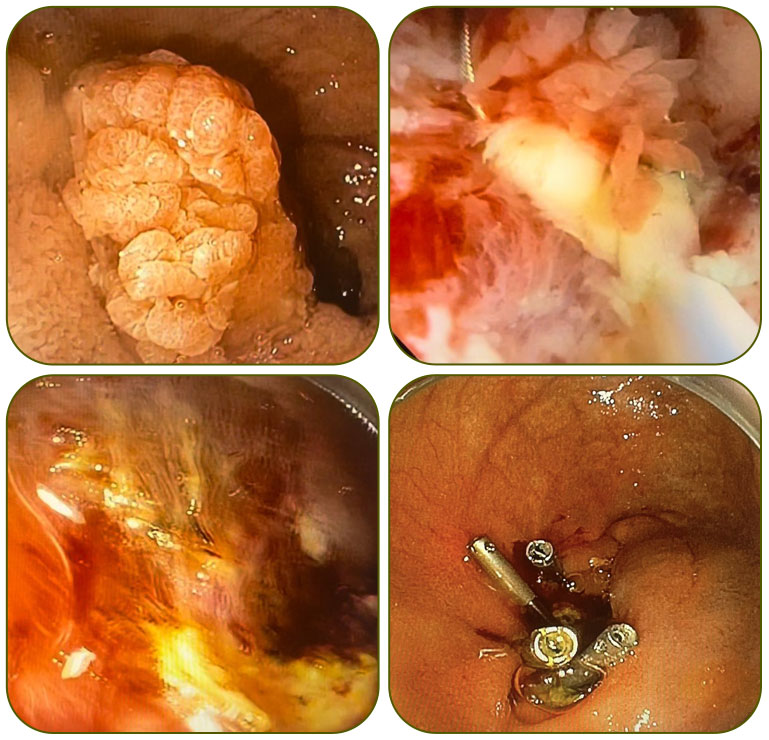
Huge fundic adenomatous lesion (>15 cm) in a 75-year-old high-risk patient was successfully treated with ESD (Endoscopic Submucosal Dissection), followed by endoscopic suturing.
EUS guided Coiling and glue injection for bleeding gastric varix
One of the most difficult locations for ESD performed regularly by Dr Patra, with very high success rates.
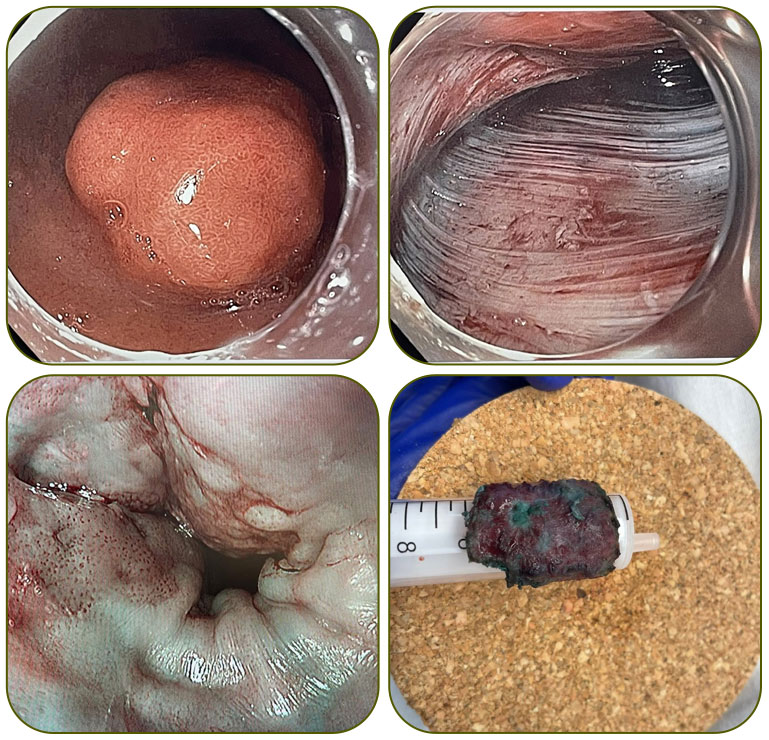
The ultimate work of art for a third-space endoscopist: a clean ESD resection base and a well-mounted en bloc specimen.
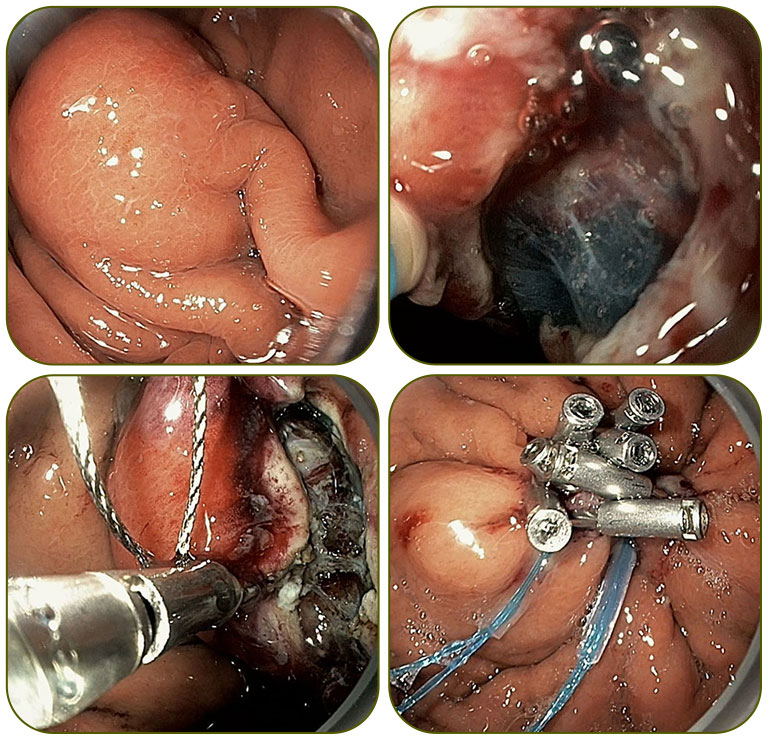
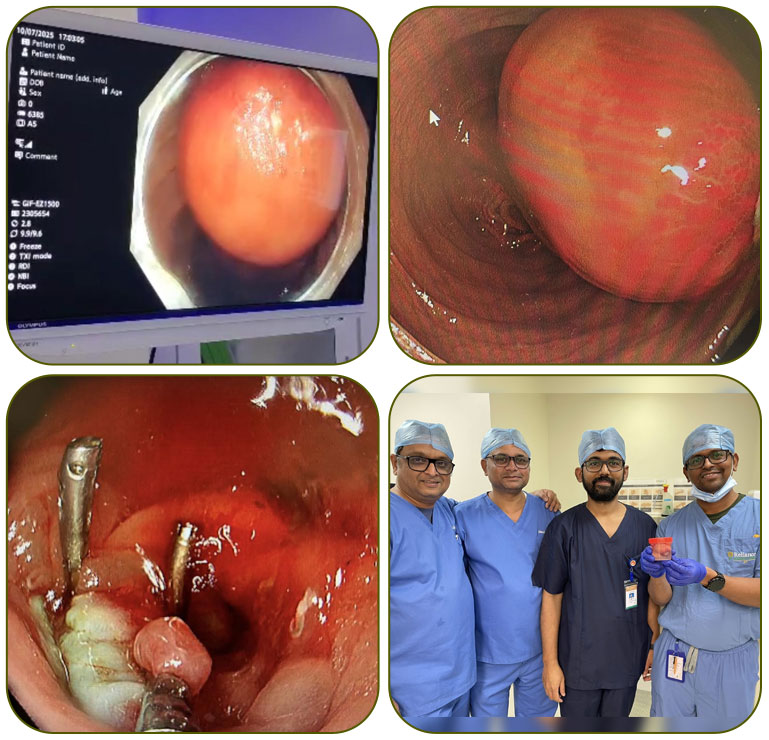
Endoscopic resection of a 3 cm GIST from an extremely difficult location – the gastric fundus, anterior wall toward the lateral greater curvature.
Proud to have participated in the British Society of Gastroenterology (BSG) Endo Bridge 2026, as part of the Indian team and demonstrated multiple live cases.

A large circumferential rectal tumor starting from the anal verge, with extensive fibrosis and dense vascularity, was successfully removed with Endoscopic Submucosal Dissection (ESD) and partial Endoscopic Intermuscular Dissection (EID).
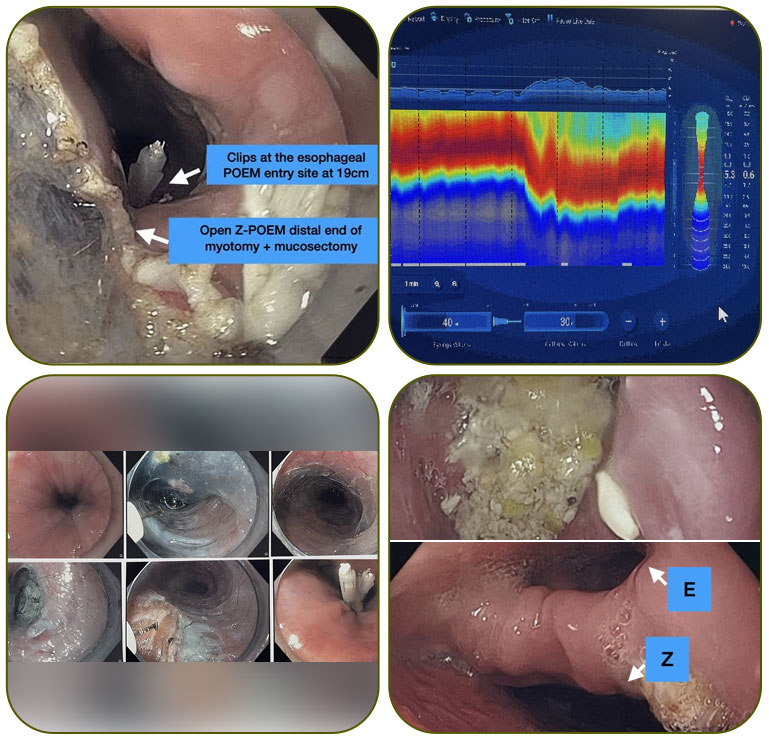
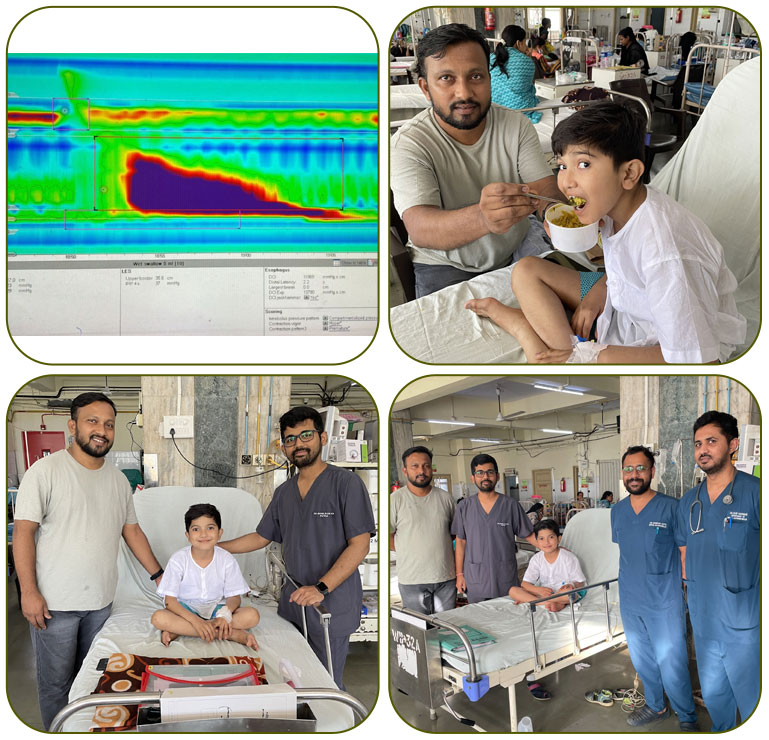
Near-complete esophageal myotomy in a single session!
An exceptional case where almost the entire esophagus underwent myotomy, sparing just a 2–3 cm segment in between.
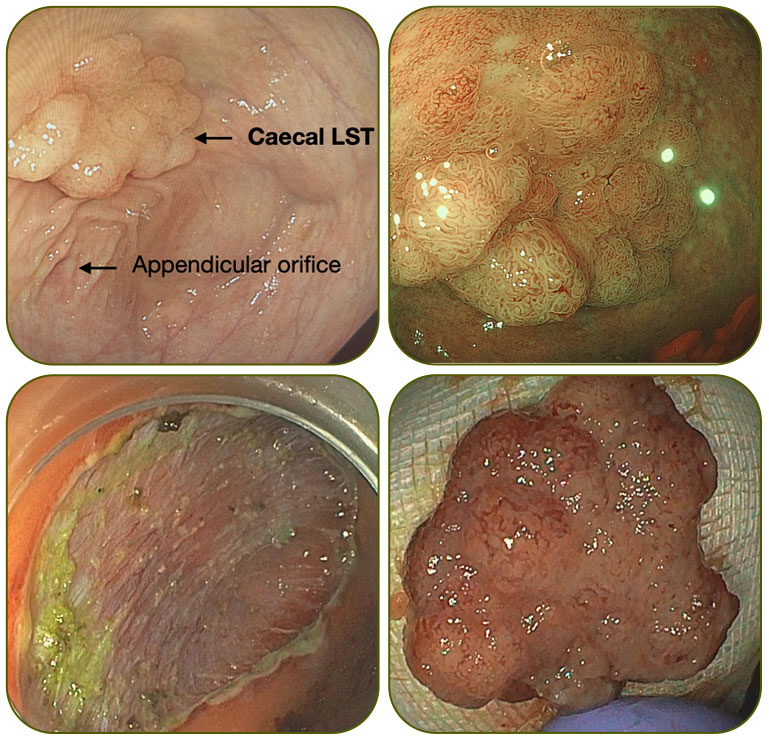
Performed 7 ESDs, including high-risk cases such as cecal LST (4 cm), rectosigmoid recurrence (4 cm), hepatic flexure lesion (6 cm), giant D1 tumor (12 cm), and D2 NET, along with 5 POEM procedures for Achalasia Cardia (sigmoid, redo, anterior).
Challenging case: Post-LAR status (for rectal adenocarcinoma) with recurrence at the anastomotic site, presenting as a 7 × 4 cm LST with a nodular component. Extensive fibrosis with 6–7 surgical clips in the dissection plane. En bloc resection was successfully achieved.
Multiple ESDs, difficult EMRs, and POEMs performed successfully, including Duodenal NET (2.5 cm), giant transverse colon lipoma (7–8 cm), circumferential esophageal ESD with curative R0 resection, two rectal ESDs, two difficult EMRs, and three POEMs.
Duodenal ESD: Once the toughest challenge, now a routine at our centre.
Transverse colon lipoma (8x7cm) causing intussusception with intermittent obstruction.
“Complex Polyp? Difficult Location? Flawless EMR Success.”
Turning Extreme Difficulty into Perfect Precision.
Cutting-edge care : Underwater EMR of a D3–D4 duodenal lesion.
"Submerge & Surge: Faster, safer duodenal lesion removal."
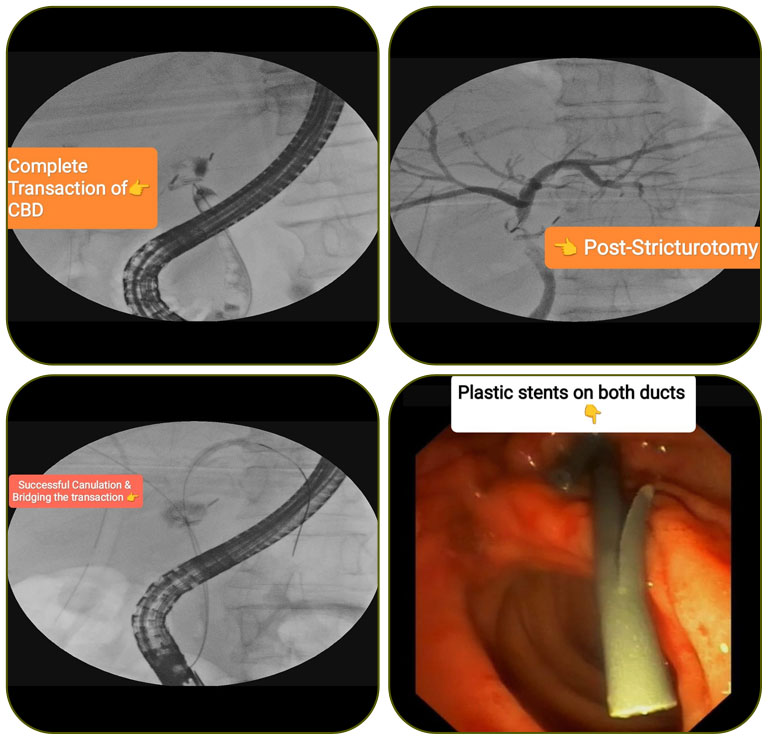
“Cutting-edge care: Cholangioscopy guided Thulium LASER Recannalisation of a total bile duct transection”
Precision in early detection meets precise removal — NBI, high-resolution scope, and ESD.

Circumferential ESD (6 cm) with en bloc resection performed successfully in a high-risk 74-year-old cirrhotic patient with esophageal varices, coagulopathy, and multiple comorbidities—without any bleeding or DMI.
EndoFLIP + POEM: Cutting-edge clarity for every myotomy.

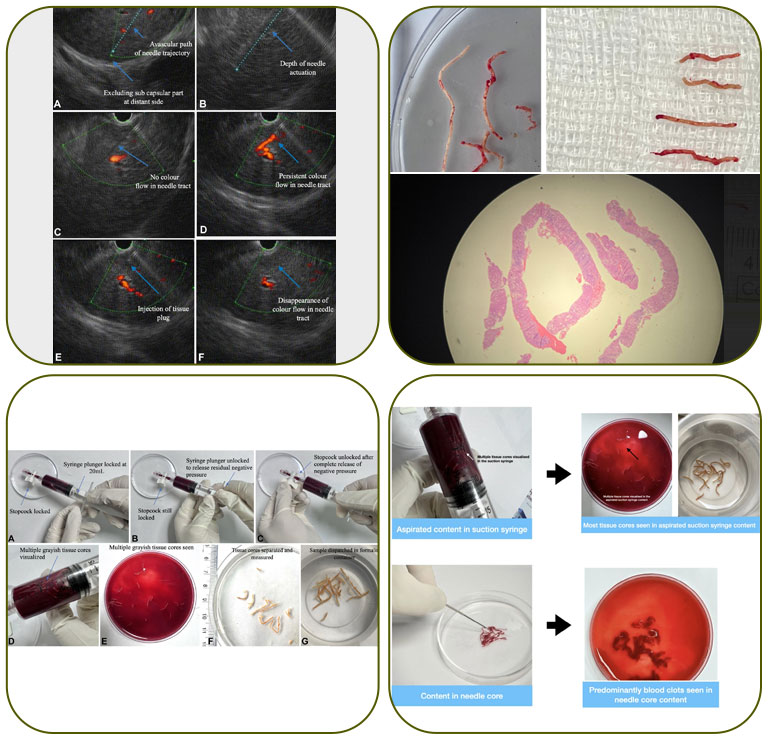
EUS guided Liver Biopsy: multiple innovative techniques described and published in international journals.
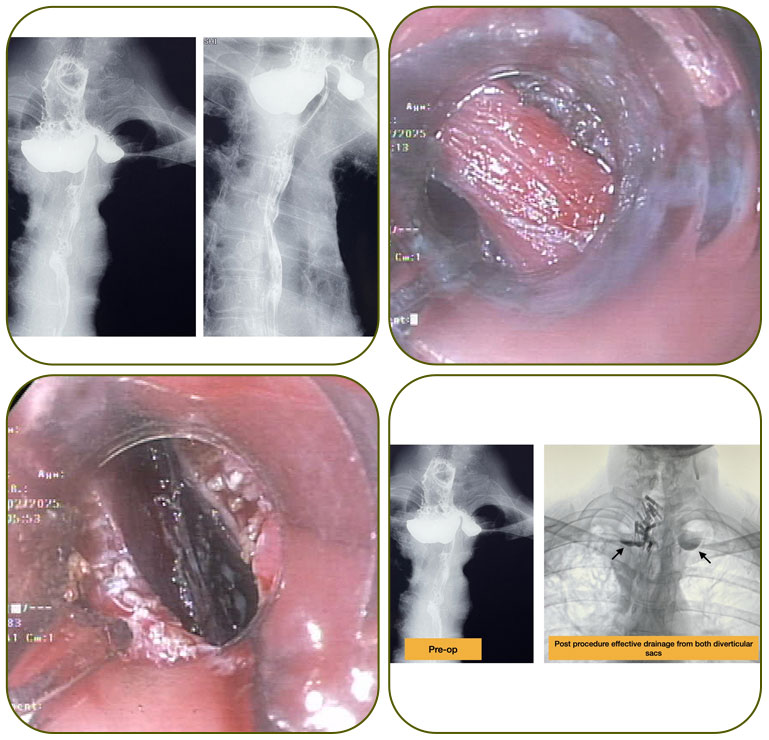
Bilobed Zenker’s diverticulum (large, 6cm) with superimposed corrosive injury to diverticular mucosa with multiple pseudodiverticulosis.
No external wound or cut, tumor removed by endoscopic surgery through the mouth
Completely removed with great success.

One of the difficult cases, successfully performed, great outcome.
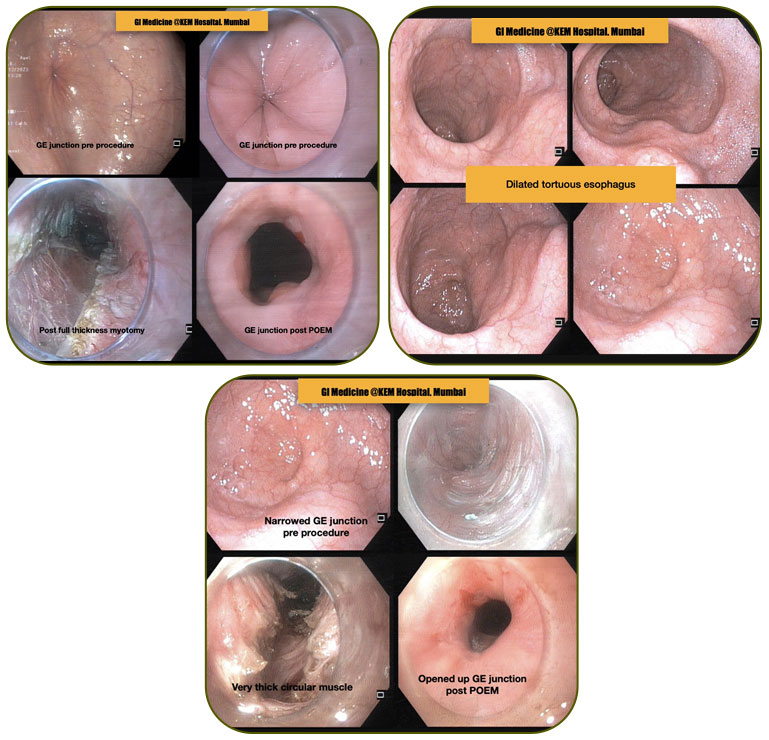
Multiple complicated POEM: Sigmoid esophagus, redo and failed POEM, anterior POEM
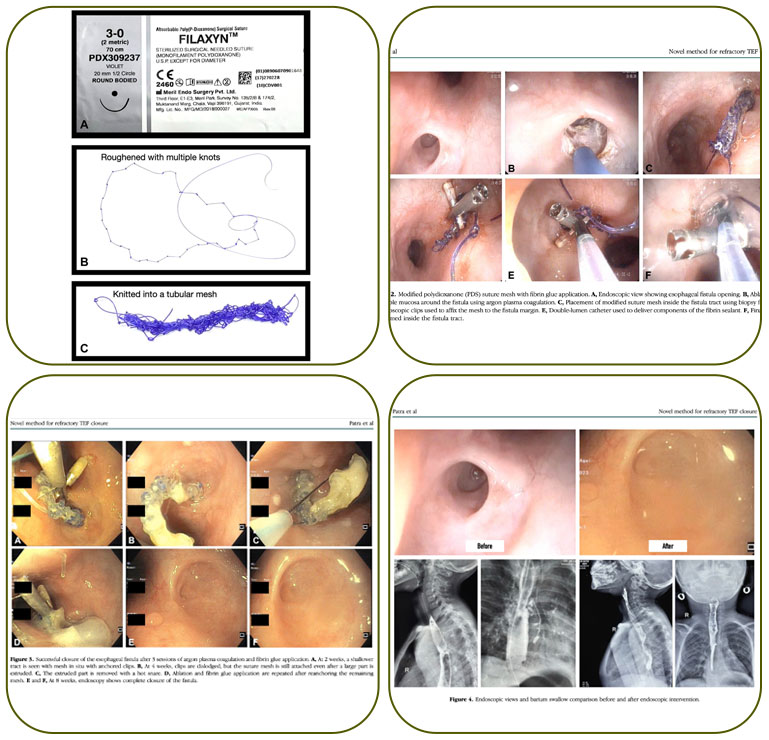
Innovation: Multiple GI Fistula, new techniques described and published with successful outcome
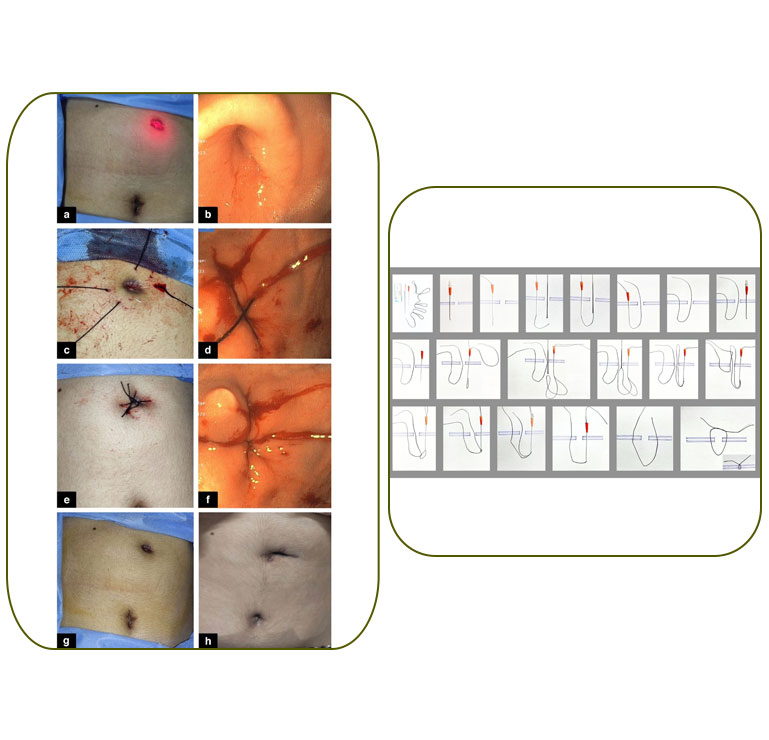
Gastroscopy-guided percutaneous suturing for closure of persistent gastrocutaneous fistula: A novel and cost-effective method